Immune Reconstitution Inflammatory Syndrome (IRIS) is defined as worsening of a preexisting untreated or partially treated opportunistic infection or appearance of a previously unrecognized opportunistic infection following immune restoration of an immunocompromised individual. It is most commonly seen in HIV infected individuals following initiation of effective combination anti-retroviral therapy (cART). But it may also be seen in other causes of immunocompromised status including organ donor recipients
Types of IRIS
Paradoxical IRIS
Worsening of a previously treated or partially treated opportunistic infection
Unmasking IRIS
Manifestation of a previously unrecognized opportunistic infection
Etiological Classification
Infective
- Bacterial
- Mycobacterium Tuberculosis
- Mycobacterium Avium Complex
- Whipple's Disease
- Viral
- Cytomegalovirus
- Viral Hepatitis
- Progressive Multifocal Leucoencephalopathy (PMLE)
- Herpes Zoster
- Fungal
- Pneumocystis
- Cryptococcus
- Histoplasma
Auto-immune
- Guillain-Barré Syndrome
- Sarcoidosis
Malignant
- Kaposi's Sarcoma
- Non-Hodgkin Lymphoma
TB IRIS
Tuberculosis associated IRIS is the condition in which tubercular infection which has been previously unrecognized or which has been well-responding to treatment, but shows worsening of clinical condition after initiation of anti-retroviral therapy (ART). The symptoms may include —
- Fever
- Cough
- Lymphadenopathy
- Pleural effusion
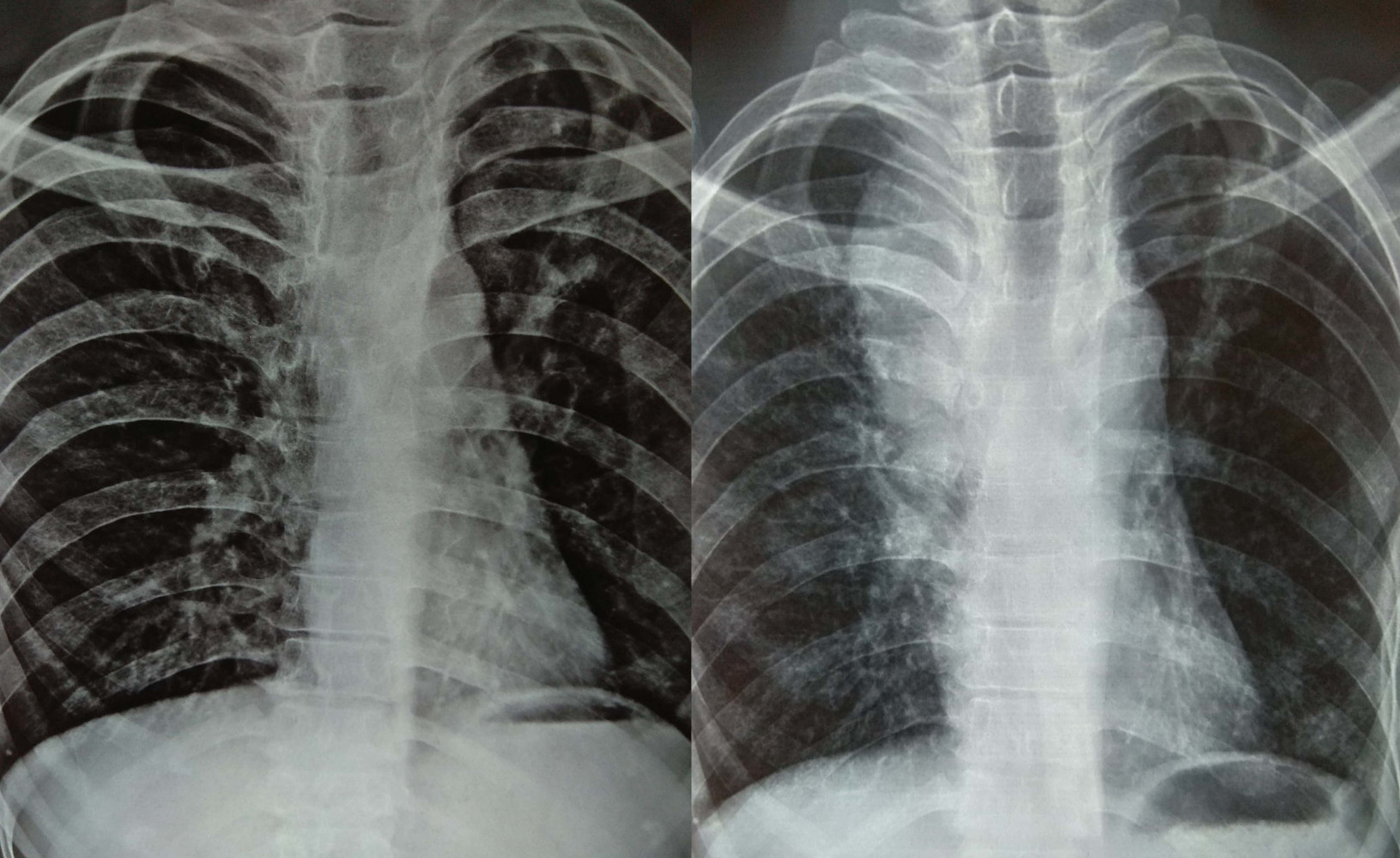
- X-ray abnormalities
TB IRIS is more common in the following conditions —
- Advanced AIDS (CD4 < 50)
- Disseminated TB / Extra-Pulmonary TB
- Good response to ART
- Early ART initiation
TB IRIS is usually seen within 1-3 months of ART initiation. It is usually self-limiting and mortality is rare. In India the incidence of TB IRIS is around 51.3/person-yearsjiapac1
Defnitions
French et al, 2004
- Major criteriafrench
- Atypical presentation of OI in ART responsive patient
- Localized disease
- Exaggerated inflammation
- Atypical inflammation
- Worsening after improvement with specific therapy after ART excluding toxicity / new diagnosis
- Decreased plasma HIV RNA by > 1log10 copies/ml
- Atypical presentation of OI in ART responsive patient
- Minor criteria
- Increased CD4 after ART
- Increased immune response to pathogen
- Spontaneous resolution
Diagnosis requires any of the following —
- Two major criteria
- One major + two minor criteria
Shelburne et al, 2006
- HIV infected patientshelburne
- Receiving effective ART as evidenced by
- Decreased HIV RNA from baseline
- Increased CD4 from baseline
- Consistent clinical symptoms
- Inconsistent clinical course
Colebunders et al, 2006
- Suspected TB IRIScolebunders
- Initial clinical response to TB treatment
- New clinical symptoms (no other identifiable cause)
- Persistent fever, worsening dyspnea, stridor, increased lymph node size, abscess, abdominal pain, retroperitoneal lymph nodes (RPLN), central nervous system symptoms etc.
- Adequate adherence to ART and ATD
- Confirmed TB IRIS
- Worsening radiologic findings
- Intrathoracic lymphadenopathy, pulmonary infiltrates, pleural effusion, RPLN, hepatosplenomegaly
- Response to ART, evidenced by any of the following
- Virological response
- Increased CD4
- Tuberculin test negative to positive
- Adequate adherence to ATD and ART
- Exclusion of other conditions including
- ATD failure
- Concomitant infections, tumors or allergies
- Worsening radiologic findings
Proposed definitions in resource limited settings
These definitions were proposed in a meeting at Kampala, Uganda in November, 2006 which was attended by 97 researchers from 16 countries on 6 continents. They were published in a paper in Lancet Infectious Disease in August, 2008.lancet1
Paradoxical TB IRIS
- Antecedent criteria, requires both
- TB diagnosis before starting ART
- Initial response to ATD
- Clinical criteria
- Within 3 months of ART
- One major or two minor (new/worsening)
- Major criteria
- Lymph node, abscess, focal involvement
- Radiological finding
- CNS TB
- Serosistis
- Minor criteria
- Constitutional symptoms
- Respiratory symptoms
- Abdominal pain with peritonitis, hepatomegaly, splenomegaly or RPLN
- Exclusion criteria
- ATD failure
- Poor adherence to ATD
- Another OI or neoplasm
- Drug toxicity or reaction
ART associated TB
- Not receiving ATD when ART is initiated
- Active TB diagnosed after ART initiation
- TB diagnosis fulfils WHO criteria
Unmasking TB IRIS
- Not receiving ATD when ART is initiated
- Presents with active TB within 3 months of ART
- And, one of the following
- Heightened clinical manifestations
- Paradoxical reaction after ATD
Management of TB IRIS
- Continuation of ATD and ART
- NSAIDS for symptomatic management
- Corticosteroids for severe manifestations
- Prednisolone 1mg/kg/day, in tapering dose
Links
References
- Nisha Thambuchetty, Kayur Mehta, Karthika Arumugam, Umadevi G. Shekarappa, Jyothi Idiculla and Anita Shet. The Epidemiology of IRIS in Southern India: An Observational Cohort Study. Journal of the International Association of Providers of AIDS Care. 2017 Sep-Oct; 16(5): 475–480
- French MA, Price P, Stone SF. Immune restoration disease after antiretroviral therapy. AIDS. 2004; 18:1615–27. [PubMed: 15280772]
- Shelburne SA, Montes M, Hamill RJ. Immune reconstitution inflammatory syndrome: more answers, more questions. J Antimicrob Chemother. 2006; 57:167–70. [PubMed: 16354748]
- Colebunders R, John L, Huyst V, Kambugu A, Scano F, Lynen L. Tuberculosis immune reconstitution inflammatory syndrome in countries with limited resources. Int J Tuberc Lung Dis. 2006; 10:946–53. [PubMed: 16964782]
- Graeme Meintjes, Stephen D Lawn, Fabio Scano, Gary Maartens, Martyn A French, William Worodria, Julian H Elliott, David Murdoch, Robert J Wilkinson, Catherine Seyler, Laurence, John, Maarten Schim van der Loeff, Peter Reiss, Lut Lynen, Edward N Janoff, Charles Gilks and Robert Colebunders. Tuberculosis-associated immune reconstitution inflammatory syndrome: case definitions for use in resource-limited settings. Lancet Infectious Disease. 2008 August ; 8(8): 516–523
 RSS Feed
RSS Feed
Write a comment: