Hypoxia is usually accompanied by respiratory distress which frequently helps in evaluation of hypoxic patients in clinical settings. However, the recent pandemic of COVID-19 has shown that this common occurrence may be challenged in some cases such as patients having profound hypoxia even without any complaint of dyspnea.
Absence of sensation of dyspnea or signs of respiratory distress even in presence of profound arterial hypoxemia is known as Happy Hypoxia or Silent Hypoxia.
Happy hypoxia has been observed as a common feature of COVID-19 pneumonia. But several other disease conditions may also have this feature including atelectasis, intrapulmonary shunt, intracardiac shunt etc.
Sensation of dyspnea
Sensation of dyspnea is controlled by the respiratory center located in the medulla oblongata and pons region of the brainstem. There are various stimuli that can regulate the respirationganong —
| Chemical Control | Non-chemical control | ||||
|---|---|---|---|---|---|
|
|
Oxygen hemoglobin dissociation curve
In COVID-19, hypoxemia may result in increased ventilation resulting in CO2 washout. The drop in CO2 results in respiratory alkalosis which shifts the oxygen hemoglobin dissociation curve towards the left. This translates to a higher affinity of Hb to O2. As a result SP2 may remain high even in the presence of profound arterial hypoxemia.dhont20
For this reason, monitoring patients by SpO2 alone may result in a false sense of security whereas an arterial blood gas analysis (ABG) may reveal underlying arterial hypoxemia.
Hypoxemia in COVID-19
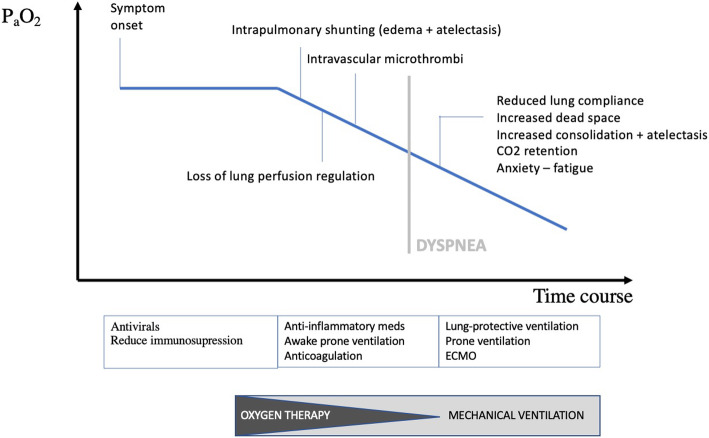
Courtesy: Dhont et al. Respir Res. (CC BY 4.0)
Arterial hypoxemia in COVID-19 may occur via multiple mechanismsdhont20 —
| Intrapulmonary shunting | In early course of the disease alveolar collapse may occur due to increased lung edema, loss of surfactant and superimposed pressure. Continued perfusion of these collapsed alveoli effectively results in intrapulmonary shunting and V/Q mismatch. |
| Loss of lung perfusion regulation | Hypoxic pulmonary vasoconstriction mechanism is responsible for reducing the blood flow to the non-aerated part of the lung and thereby maintaining the V/Q ratio. However, this mechanism fails in COVID-19, possibly due to cytokines. |
| Intravascular microthrombi | SARS-COV-2 damages the ACE-2 expressing endothelial cells. In this background microthrombi may form due to an imbalance between procoagulant and fibrinolytic activities. Pulmonary arterial thrombosis and embolism further worsens the V/Q mismatch in COVID-19. |
| Impaired diffusion capacity | SARS-COV-2 invades and damages the type II alveolar cells. Loss of alveolar epithelial cells and the procoagulant state results in deposition of fibrin, dead cells and complement activation products over the denuded basement membrane which is called hyaline membrane. It impairs gas diffusion across the alveolar membrane and causes an increase of P(A-a)O2 gradient. |
Preserved lung mechanics
In some patients, gas exchange abnormalities occur earlier than increase in mechanical load of lung. During initial period of COVID-19 lung mechanics are mostly preserved despite arterial hypoxemia. In early period following features may be observeddhont20 —
- No increased airway resistance.
- No increase in physiological or anatomical dead space.
- Normal lung compliance, hence no increased breathing effort.
Neural hypothesis
Carotid body contains chemoreceptors which are activated by decreased PaO2. This afferent signal is relayed to the nucleus tractus solitarius via glossopharyngeal nerve.
A hypothesis has been proposed that the invasion of the carotid body receptorssimonson20 or nucleus tractus solitariusanoop20 itself may result in an impaired response of the respiratory center to the arterial hypoxemia in COVID-19.
False sense of security
However, happy hypoxia is a temporary phenomenon. As disease progresses and further lung involvement occurs, dyspnea appears in these patients.dhont20
- Total lung compliance is reduced as more and more alveoli collapse resulting in increased work of breathing.
- Dynamic compliance may also reduce due to loss of surfactant, increasing work of breathing.
- Intravascular thrombi may cause reduced lung perfusion and thereby increasing physiological dead space.
- Anxiety may also cause dyspnea by means of cortical feedback to the respiratory center.
L-type vs H-type
COVID-19 pneumonia may present with two phenotypesgattinoni20 —
| L-type | H-type |
|---|---|
|
|
Progression of the disease is often associated with the transition of type L to type H pneumonia.
Conclusion
Although dyspnea may be absent during the initial phase of COVID-19 pneumonia, arterial hypoxemia needs to be monitored with ABG. Rapid deterioration may occur and the patient may rapidly progress from happy hypoxia to overt dyspnea at short notice.
- Barrett EK et al. Ganong's Review of Medical Physiology. Ed 25th. USA. McGrawHill. 2016.
- Dhont S et al. The pathophysiology of ‘happy’ hypoxemia in COVID-19. Respir Res. 2020; 21: 198. https://doi.org/10.1186/s12931-020-01462-5
- Anoop UR et al. Happy Hypoxemia in COVID-19-A Neural Hypothesis. ACS Chem Neurosci. 2020 Jul 1;11(13):1865-1867. https://doi.org/10.1021/acschemneuro.0c00318
- Simonson TS et al. Silent hypoxaemia in COVID-19 patients. J Physiol. 2020 Dec 21. https://doi.org/10.1113/JP280769
- Gattinoni L et al. COVID-19 pneumonia: different respiratory treatments for different phenotypes? Intensive Care Med. 2020 Jun;46(6):1099-1102. https://doi.org/10.1007/s00134-020-06033-2
 RSS Feed
RSS Feed
Write a comment: